
Cannabis probably causes schizophrenia
But the data are less decisive than we would like

A lot of countries are currently pondering whether they should legalize or decriminalize the sale of cannabis for recreational use. Cannabis is generally considered a fairly safe drug, at least, insofar as acute dangers are concerned. Overdosing by ordinary use is impossible. However, there are long-running associations between cannabis use and schizophrenia. There are 1000s of studies trying to figure out if this relationship is causal or due to some kind of confounding. The question has some public policy relevance insofar as legalization is likely to increase the use of cannabis. If cannabis use causes schizophrenia, this will then lead to some increase of schizophrenia cases. Schizophrenia is extremely expensive -- lifetime cost of about 1M in an Australian study -- to society because schizophrenics need treatment, are very violent, and not very good on the job market. Overall, then, they are a large net negative on the state's budgets. If this increased spending is to be covered by the sale of cannabis, one has to add a tax that corresponds to this increased spending. Hence, the need to know about the causality.
So what can we do? Of course, anyone can run the usual longitudinal studies. One can show that cannabis use usually precedes a schizophrenia diagnosis. But this doesn't tell us whether cannabis use caused schizophrenia because it is possible that latent/liability for schizophrenia makes people smoke cannabis. In other words, the problem is between these causal models:
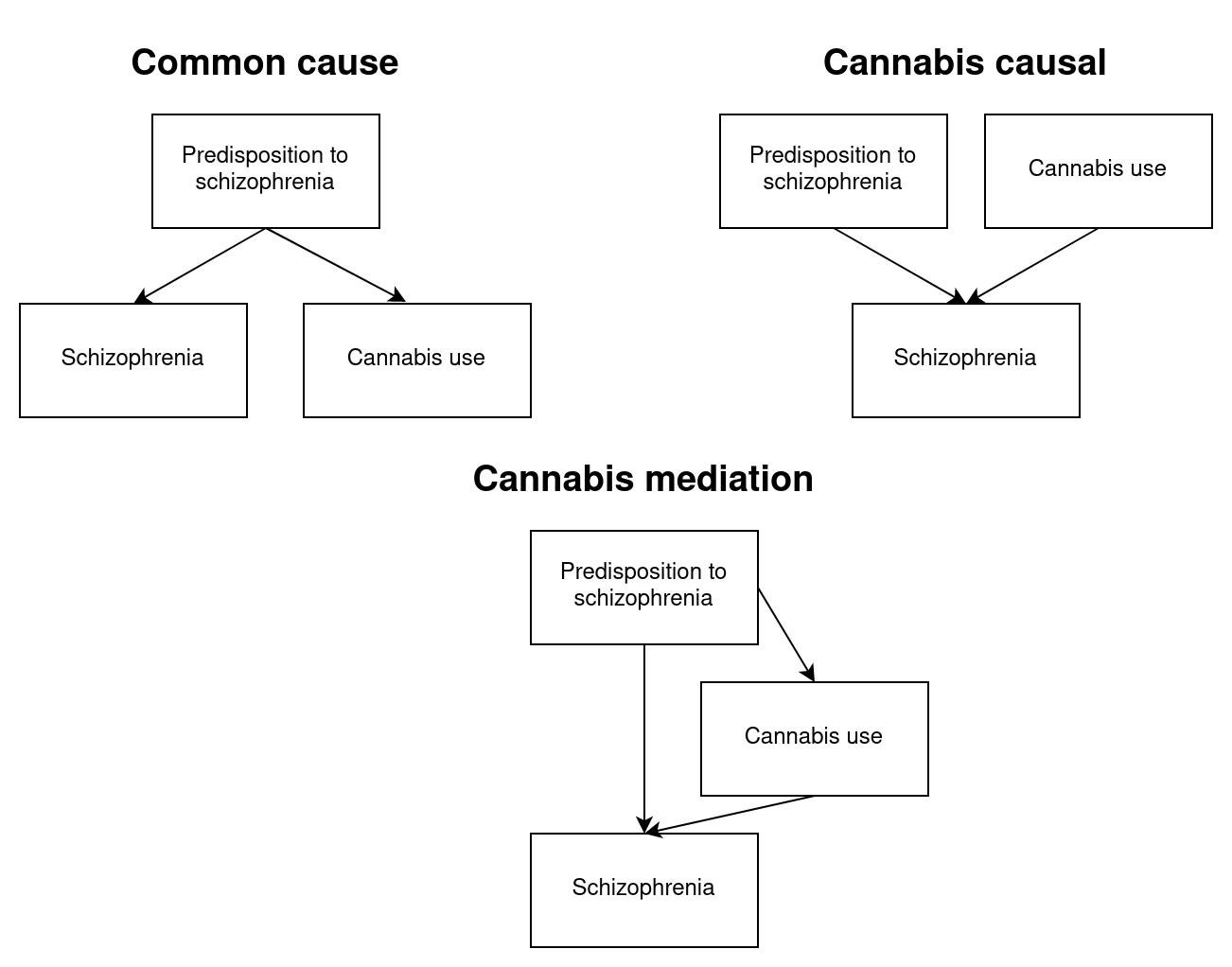
More complicated models are possible (say, schizophrenia also causing cannabis use), but from a policy perspective, the main difference is between model 1, where cannabis is not causal but a proxy for predisposition, and models 2 and 3, where cannabis is causal.
So how do we tell? Of course, we could theoretically assign some thousands of people to either smoke or not smoke cannabis for 10 years and see if there's any difference in their ratios of schizophrenia. Since this kind of trial is out of the question, we are left with trying to figure out causality from various indirect methods. What about family studies? The idea here being that a predisposition to schizophrenia is going to be mostly a matter of genetics, and if so, that means we can use family members to see if genetic confounding can account for all of the association we see between (prior) cannabis use and schizophrenia. If it cannot, then this is decent evidence of causality. First, however, the assumption that it is mostly a matter of genetics. Here's a recent Nordic register study:
Methods Combining two nationwide registers, the Danish Twin Register and the Danish Psychiatric Research Register, we identified a sample of twins born between 1951 and 2000 (N = 31,524 twin pairs). Twins were followed until June 1, 2011. Liability threshold models adjusting for censoring with inverse probability weighting were used to estimate probandwise concordance rates and heritability of the diagnoses of SZ and SZ spectrum disorders.
Results The probandwise concordance rate of SZ is 33% in monozygotic twins and 7% in dizygotic twins. We estimated the heritability of SZ to be 79%. When expanding illness outcome to include SZ spectrum disorders, the heritability estimate was almost similar (73%).
We see the usual finding of no detectable effect of the family environment, and a dominant genetic component. As the diagnosis has some random error and because assortative mating is not accounted for, these heritabilities are a bit too low. We can probably assume about 90% genetics and 10% randomness.
Based on this, we know that all the familial confounding is genetic in origin, and we have to account for this in the studies that measure cannabis use and schizophrenia. I am aware of 4 studies that tried to do this:
Giordano, G. N., Ohlsson, H., Sundquist, K., Sundquist, J., & Kendler, K. S. (2015). The association between cannabis abuse and subsequent schizophrenia: a Swedish national co-relative control study. Psychological medicine, 45(2), 407-414.
Background Although cannabis abuse (CA) is known to be associated with schizophrenia, the causal nature of this association is unclear, with prodromal effects complicating its interpretation.
Method From Swedish national registry databases, we used a co-relative case–control design with full-sibling, half-sibling and first-cousin comparisons, alongside a general Swedish population sample. Using ICD codes, 5456 individuals with an initial diagnosis of schizophrenia (2000–2010) were matched with five schizophrenia-free controls. We further identified first-cousin, half-sibling and full-sibling pairs discordant for CA and statistically extrapolated results for discordant monozygotic (MZ) twins.
Results Within the general Swedish population, CA was strongly associated with later schizophrenia [odds ratio (OR) 10.44, 95% confidence interval (CI) 8.99–12.11]. This association was substantially attenuated both by increasing temporal delays between CA exposure and schizophrenia diagnosis and by controlling for increasing degrees of familial confounding. Extrapolated discordant MZ pairs suggested that fully controlling for confounding familial factors reduced the association between CA and later schizophrenia to more modest levels (ORs of approximately 3.3 and 1.6 with 3- and 7-year temporal delays respectively). Opiate, sedative, cocaine/stimulant and hallucinogen abuse were also strongly associated with subsequent schizophrenia in the general population. After controlling for familial confounding, only cocaine/stimulant exposure remained associated.
Nesvåg, R., Reichborn-Kjennerud, T., Gillespie, N. A., Knudsen, G. P., Bramness, J. G., Kendler, K. S., & Ystrom, E. (2017). Genetic and environmental contributions to the association between cannabis use and psychotic-like experiences in young adult twins. Schizophrenia Bulletin, 43(3), 644-653.
To investigate contributions of genetic and environmental risk factors and possible direction of causation for the relationship between symptoms of cannabis use disorders (CUD) and psychotic-like experiences (PLEs), a population-based sample of 2793 young adult twins (63.5% female, mean [range] age 28.2 [19–36] y) were assessed for symptoms of CUD and PLEs using the Composite International Diagnostic Interview. Latent risk of having symptoms of CUD or PLEs was modeled using Item Response Theory. Co-twin control analysis was performed to investigate effect of familiar confounding for the association between symptoms of CUD and PLEs. Biometric twin models were fitted to estimate the heritability, genetic and environmental correlations, and direction for the association. Lifetime use of cannabis was reported by 10.4 % of the twins, and prevalence of PLEs ranged from 0.1% to 2.2%. The incidence rate ratio of PLEs due to symptoms of CUD was 6.3 (95% CI, 3.9, 10.2) in the total sample and 3.5 (95% CI, 1.5, 8.2) within twin pairs. Heritability estimates for symptoms of CUD were 88% in men and women, and for PLEs 77% in men and 43% in women. The genetic and environmental correlations between symptoms of CUD and PLEs were 0.55 and 0.52, respectively. The model allowing symptoms of CUD to cause PLEs had a better fit than models specifying opposite or reciprocal directions of causation. The association between symptoms of CUD and PLEs is explained by shared genetic and environmental factors and direct effects from CUD to risk for PLEs.
Karcher, N. R., Barch, D. M., Demers, C. H., Baranger, D. A., Heath, A. C., Lynskey, M. T., & Agrawal, A. (2019). Genetic predisposition vs individual-specific processes in the association between psychotic-like experiences and cannabis use. JAMA psychiatry, 76(1), 87-94.
Design, Setting, and Participants In this cross-sectional analysis, diagnostic interviews and self-reported data were collected from 2 separate population-based samples of twin and nontwin sibling pairs. Data from the Human Connectome Project were collected between August 10, 2012, and September 29, 2015, and data from the Australian Twin Registry Cohort 3 (ATR3) were collected between August 1, 2005, and August 31, 2010. Data were analyzed between August 17, 2017, and July 6, 2018. The study included data from 1188 Human Connectome Project participants and 3486 ATR3 participants, totaling 4674 participants.
Main Outcomes and Measures Three cannabis-involvement variables were examined: frequent use (ie, ≥100 times), a DSM-IV lifetime cannabis use disorder diagnosis, and current cannabis use. Genetic and environmental correlations between cannabis involvement and PLEs were estimated. Generalized linear mixed models examined PLE differences in twin and nontwin sibling pairs discordant for cannabis use.
Results Among the 4674 participants, the mean (SD) age was 30.5 (3.2) years, and 2923 (62.5%) were female. Data on race/ethnicity were not included as a covariate owing to lack of variability within the ATR3 sample; among the 1188 participants in the Human Connectome Project, 875 (73.7%) were white. Psychotic-like experiences were associated with frequent cannabis use (β = 0.11; 95% CI, 0.08-0.14), cannabis use disorder (β = 0.13; 95% CI, 0.09-0.16), and current cannabis use (β = 0.07; 95% CI, 0.04-0.10) even after adjustment for covariates. Correlated genetic factors explained between 69.2% and 84.1% of this observed association. Within discordant pairs of twins/siblings (Npairs, 308-324), Psychotic-like experiences were more common in cannabis-exposed individuals compared with their relative who used cannabis to a lesser degree (β ≥ .23, P < .05; eg, frequent and infrequent cannabis-using relatives significantly differed, z = −5.41; P < .001).
Conclusions and Relevance Despite the strong contribution of shared genetic factors, frequent and problem cannabis use also appears to be associated with PLEs via person-specific pathways. This study’s findings suggest that policy discussions surrounding legalization should consider the influence of escalations in cannabis use on traitlike indices of vulnerability, such as PLEs, which could contribute to pervasive psychological and interpersonal burden.
Schaefer, J. D., Hamdi, N. R., Malone, S. M., Vrieze, S., Wilson, S., McGue, M., & Iacono, W. G. (2021). Associations between adolescent cannabis use and young-adult functioning in three longitudinal twin studies. Proceedings of the National Academy of Sciences, 118(14), e2013180118.
Observational studies have linked cannabis use to an array of negative outcomes, including psychiatric symptoms, cognitive impairment, and educational and occupational underachievement. These associations are particularly strong when cannabis use occurs in adolescence. Nevertheless, causality remains unclear. The purpose of the present study was thus to examine associations between prospectively assessed adolescent cannabis use and young-adult outcomes (psychiatric, cognitive, and socioeconomic) in three longitudinal studies of twins (n = 3,762). Twins reporting greater cumulative cannabis use in adolescence reported higher levels of psychopathology as well as poorer socioeconomic outcomes in young adulthood. However, cannabis use remained associated only with socioeconomic outcomes (i.e., educational attainment, occupational status, and income) in monozygotic-cotwin control analyses, which account fully for shared genetic and environmental confounding. Follow-up analyses examining associations between twin differences in adolescent cannabis use and longitudinal change in academic functioning during the middle- and high-school years provided a possible mechanism for these associations, indicating that greater cannabis use during this period was associated with decreases in grade point average and academic motivation as well as increases in academic problem behavior and school disciplinary problems. Our findings thus suggest that cannabis use in adolescence has potentially causal, deleterious effects on adolescent academic functioning and young-adult socioeconomic outcomes despite little evidence suggesting a strong, causal influence on adult mental health or cognitive ability.
So 3 studies suggest some causality, but the newest study suggests maybe not. We can guess at what the problems might be. Let's begin with Giordano. This study didn't actually use mono-zygotic twins, but rather used various different family members of known relationship. By seeing how much the association between pre-onset cannabis use and schizophrenia associate in the various groups, one can estimate the association in the unobserved MZ group. They found this association was about half that of the general population:
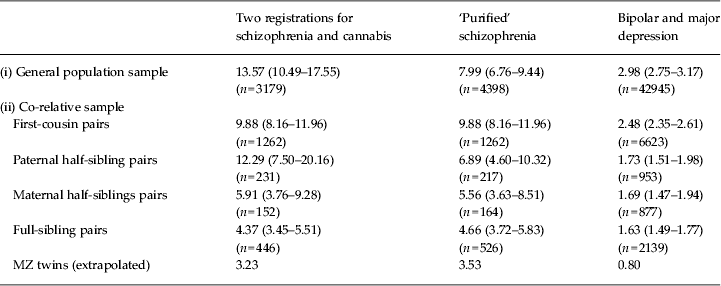
Thus, in the general population, the association was about 8 (OR) and in the extrapolated MZ group, it was 3.5 (numbers from middle column). This suggests about half the relationship is due to genetic confounding and the rest is causal. To hone in a causality, they show that the same analysis for other drugs yield near 0 associations in the MZ group, highlighting the role of cannabis in particular (cocaine/amphetamine was also possibly causal though no confidence intervals are given).
In the Nesvåg study, they had access to actual MZ twins, and were able to do a regular MZ control design. Their fitting showed about the same as the above, with about half the association being accounted for by the familial confounding ("The incidence rate ratio of PLEs due to symptoms of CUD was 6.3 (95% CI, 3.9, 10.2) in the total sample and 3.5 (95% CI, 1.5, 8.2) within twin pairs."). The main issue here is that it didn't study schizophrenia per se, but rather "psychotic-like experiences" (having a psychotic episode) which I take to be a good proxy. They additionally did some model fitting comparison to see whether a cannabis causing schizophrenia model fitted better than the alternative, finding it did.
In the Karcher study, they did much the same as Nesvåg, studying PLE instead of schizophrenia. Their results show a rather lower heritability of PLE of 38% compared to "77% in men and 43% in women" in Nesvåg. This much lower heritability makes me think maybe the PLE construct isn't such a good proxy, or at least has a lot of measurement error. They also used discordant twins (twin control) to see if cannabis use was potentially causal for PLE, finding that it was. However, their effect size between twins was about twice that of the general population (in MZs beta = 0.23, in general population beta = 0.11). This together with the p value given as "< .05", makes me think this study overestimated the effect size due to power issues/p-hacking.
In the final study by Schaefer, they did the same kind of MZ control as above. They didn't try to extrapolate which would have given them higher power, like Giordano did. In fact, it would be best if all studies did this so we could always see whether the MZ control estimates are consistent with other family members, as a method check. But also because MZ control is usually low power because there are so few MZs in general, and because these are so similar and rarely seriously discordant for their use of cannabis. Here's their results:

You can see the problem here. The MZ estimates ("within-pair") are too noisy. Still, of their 8 tests, 3 were p < .05, and another had p = .06. This study didn't actually measure schizophrenia, but measured some other mental diagnoses. Their strongest result was that cannabis use is associated with lower educational attainment, as well as later occupational status and income. This is probably not too surprising if you know about potheads. With regards to the psychiatric outcomes, the study was underpowered. In fact, in 1 of their 4 models, the MZ analysis suggested a stronger effect size than the general population (almost the same values as the between-pair analysis above), namely for anxiety disorder (1.58 vs. 1.25). Such a result is basically impossible, so underlines the power failure here. The effect sizes were about the same within and between for depression, so that could be entirely causal, or not at all. They found no effect for IQ (vocabulary). So in general, this study looks like a null-ish result for that's an error of interpretation.
Time series
OK, if we don't have enough twins to do this research, can we at least look at some time series data? Yes. The American state Colorado legalized cannabis about a decade ago, and there's new studies of this:
Wang, G. S., Buttorff, C., Wilks, A., Schwam, D., Tung, G., & Pacula, R. L. (2022). Impact of cannabis legalization on healthcare utilization for psychosis and schizophrenia in Colorado. International Journal of Drug Policy, 104, 103685.
Background Emergency department (ED) visits involving psychosis and schizophrenia have increased at a rate exceeding population growth in the United States over the past decade. Research shows a strong dose-response relationship between chronic use of high-potency cannabis and odds of developing symptoms of psychosis. The aim of this study was to evaluate the impact of cannabis legalization on psychosis and schizophrenia-related ED visits in Colorado.
Methods Using administrative data from Colorado Hospital Association (CHA) on county-level quarterly ED visits between January 1, 2013, and December 31, 2018, we applied a difference-in-difference analysis to examine how new exposure to recreational cannabis dispensaries after 2014 differentially influenced the rate of ED visits for psychosis and schizophrenia, comparing counties with no prior medical cannabis dispensary exposure to counties with low or high medical dispensary exposure.
Results As recreational dispensaries per 10,000 residents increased, there was no significant association with the rate of schizophrenia ED visits per capita (incidence rate ratio or IRR: 0.95, 95% CI [0.69, 1.30]) while the rate of psychosis visits increased 24% (IRR: 1.24, 95% CI [1.02, 1.49]). Counties with no previous medical dispensaries experienced larger increases in schizophrenia ED visits than counties already exposed to a low level of medical dispensaries, but this effect was not significant. Counties with low baseline medical exposure had lower increases in rates of psychosis visits than counties with high baseline medical exposure (IRR 0.83, 95% CI [0.69, 0.99]).
Conclusions There was a positive association between the number of cannabis dispensaries and rates of psychosis ED visits across all counties in Colorado. Although it is unclear whether it is access to products, or the types of products that may be driving this association, our findings suggest there is a potential impact on the mental health of the local population that is observed after cannabis legalization.
They find nothing for visits to the emergency room for schizophrenia, but that strikes me as a pretty weak measure. They find a marginal hit for psychosis in general (p value looks close to .05). This study basically found nothing, and it was probably too underpowered to find what they were looking for. I didn't find any recent study for other US states that legalized a while ago (e.g. Washington).
Conclusions
Taken all together, the evidence is plausible but not conclusive. If we are to be Bayesian -- as we must -- I would guess the causality is probably in line with what the first two studies found. Most schizophrenia is caused by genetic liability (bad luck, essentially), and some small part is caused by smoking weed. Many polities have made smoking weed more common, especially among youths, so we can expect some small increase in schizophrenia rates. Since schizophrenia is fairly uncommon (lifetime prevalence 0.5-1% for Europeans), a 20% increase in cases probably won't have a noticeable effect on state finances, and would be difficult to detect unless one has a large population. Nevertheless, due to the costs associated with this, it would be wise to add a tax on such products so that their legalization doesn't harm the state budget. Drug users would then be paying for their own problems, as far as the state is concerned.
Insofar as my personal biases are concerned, I am in favor of legalization because I think the costs of the drug war are much higher than the costs of increased use from legalization, which can be offset by sales tax, and any special extra tax added to cover increased treatment costs (in socialized healthcare systems). Also, it should be recalled that most people who do drugs don't get into problems. A small minority of problem who are prone to problems already get addicted.
Extra: what about intelligence?
In one study above, there was no effect of cannabis on IQ, but the study was too small. Is there some better evidence? Yes:
Jackson, N. J., Isen, J. D., Khoddam, R., Irons, D., Tuvblad, C., Iacono, W. G., ... & Baker, L. A. (2016). Impact of adolescent marijuana use on intelligence: Results from two longitudinal twin studies. Proceedings of the National Academy of Sciences, 113(5), E500-E508.
Marijuana is one of the most commonly used drugs in the United States, and use during adolescence—when the brain is still developing—has been proposed as a cause of poorer neurocognitive outcome. Nonetheless, research on this topic is scarce and often shows conflicting results, with some studies showing detrimental effects of marijuana use on cognitive functioning and others showing no significant long-term effects. The purpose of the present study was to examine the associations of marijuana use with changes in intellectual performance in two longitudinal studies of adolescent twins (n = 789 and n = 2,277). We used a quasiexperimental approach to adjust for participants’ family background characteristics and genetic propensities, helping us to assess the causal nature of any potential associations. Standardized measures of intelligence were administered at ages 9–12 y, before marijuana involvement, and again at ages 17–20 y. Marijuana use was self-reported at the time of each cognitive assessment as well as during the intervening period. Marijuana users had lower test scores relative to nonusers and showed a significant decline in crystallized intelligence between preadolescence and late adolescence. However, there was no evidence of a dose–response relationship between frequency of use and intelligence quotient (IQ) change. Furthermore, marijuana-using twins failed to show significantly greater IQ decline relative to their abstinent siblings. Evidence from these two samples suggests that observed declines in measured IQ may not be a direct result of marijuana exposure but rather attributable to familial factors that underlie both marijuana initiation and low intellectual attainment.
Meier, M. H., Caspi, A., Danese, A., Fisher, H. L., Houts, R., Arseneault, L., & Moffitt, T. E. (2018). Associations between adolescent cannabis use and neuropsychological decline: A longitudinal co‐twin control study. Addiction, 113(2), 257-265.
Setting and Participants Participants were 1989 twins from the Environmental Risk (E-Risk) Longitudinal Twin Study, a nationally representative birth cohort of twins born in England and Wales from 1994 to 1995.
Measurements Frequency of cannabis use and cannabis dependence were assessed at age 18. Intelligence quotient (IQ) was obtained at ages 5, 12 and 18. Executive functions were assessed at age 18.
Findings Compared with adolescents who did not use cannabis, adolescents who used cannabis had lower IQ in childhood prior to cannabis initiation and lower IQ at age 18, but there was little evidence that cannabis use was associated with IQ decline from ages 12–18. For example, adolescents with cannabis dependence had age 12 and age 18 IQ scores that were 5.61 (t = −3.11, P = 0.002) and 7.34 IQ points (t = −5.27, P < 0.001) lower than adolescents without cannabis dependence, but adolescents with cannabis dependence did not show greater IQ decline from age 12–18 (t = −1.27, P = 0.20). Moreover, adolescents who used cannabis had poorer executive functions at age 18 than adolescents who did not use cannabis, but these associations were generally not apparent within twin pairs. For example, twins who used cannabis more frequently than their co-twin performed similarly to their co-twin on five of six executive function tests (Ps > 0.10). The one exception was that twins who used cannabis more frequently than their co-twin performed worse on one working memory test (Spatial Span reversed; β = −0.07, P = 0.036).
Conclusions Short-term cannabis use in adolescence does not appear to cause IQ decline or impair executive functions, even when cannabis use reaches the level of dependence. Family background factors explain why adolescent cannabis users perform worse on IQ and executive function tests.
Ross, J. M., Ellingson, J. M., Rhee, S. H., Hewitt, J. K., Corley, R. P., Lessem, J. M., & Friedman, N. P. (2020). Investigating the causal effect of cannabis use on cognitive function with a quasi-experimental co-twin design. Drug and alcohol dependence, 206, 107712.
Methods We first examined the phenotypic associations between cannabis initiation, frequency, and use disorder with cognitive abilities, while also controlling for pre-use general cognitive ability and other substance involvement. We tested the concurrent association between the cannabis use variables and cognitive abilities in late adolescence and young adulthood and the longitudinal association between cannabis use variables during adolescence and young adulthood cognitive abilities. Next, we used multilevel models to test whether these relations reflect between- and/or within-twin pair associations.
Results Phenotypically, cannabis use was related to poorer cognitive functioning, although most associations were negligible after accounting for other substance use. Nevertheless, there were few significant within-family twin-specific associations, except that age 17 cannabis frequency was associated with worse age 23 Common EF and general cognitive ability.
Conclusions We found little support for a potential causal effect of cannabis use on cognition, consistent with previous twin studies. Results suggest that cannabis use may not cause decline in cognitive ability among a normative sample of cannabis users.
So 3 twin control studies, 2 say nothing, 1 says maybe a little bit in some sub-analysis. Overall, this is probably a tiny effect and not worth caring about.

Emil, could you give an overview of research on male and female cooperation, teamwork and friendship? I'm not asking about the topic of the post, but nevertheless. I've read a lot about gender differences, but I've noticed that this topic is almost never discussed. Here's a bit of research from what I found:
https://vdare.com/posts/all-male-teams-can-succeed-without-the-teammates-liking-each-other
https://doi.org/10.1016/j.labeco.2016.09.003 https://doi.org/10.1371/journal.pone.0185408 https://doi.org/10.1016/j.actpsy.2018.04.014 https://doi.org/10.1007/s12110-014-9198-z
I know you're writing this from an European point of view. But try to think about this from the perspective of Singapore. Trafficking even small amounts of cannabis will get you the death penalty in Singapore. I can leave my cell phone at a table at Starbucks to save the seat and come back to it. Nobody will steal it. Society is much safer and cleaner when drug dealer are killed. Their genes are eliminated.
If such a law ever passes in the US, we will probably be executing at least 10K people a year if not more. Purging this many drug dealers who are likely committing other crimes will make the US much much safer and more livable. This will never happen of course. But even if we don't execute them, but we put them in prison for 30 years. That will go a long way towards isolating criminals from civil society. So no, I'm not for legalization but for tougher laws against marijuana and other drug offenses.