
Obesity and the secular decline in testosterone
Seems to be the main cause, technology to blame?

One thing I didn't address in the last post about the decline of everything manly is that obesity is a potential cause of secular declines in testosterone. That's because the relationship between obesity and testosterone in the blood is actually very strong, apparently because fat tissue absorbs it, at least, that's what the internet people claim (I wasn't able to find an academic study). Visually, it looks like this, using BMI as proxy for fat% (r = .82):

The data are from the ever relevant Vietnam Experience Study, which you can download here. It's a sample of American veterans that the US army collected to disprove claims that agent orange causes various things they would otherwise have to pay for. Jokes on them, they are paying for a lot of other stuff now. The relationship between BMI and testosterone is pretty strong and linear (blue line = nonlinear GAM fit). Age is not much of a confound here because these men are about the same age. The regression model controlling for the obvious things looks like this:

Testosterone is the outcome, the quantitative variables are standardized. The standardized beta is the same across models, even controlling for age, race, income, education, and intelligence (g). Clearly, the link from BMI to lower testosterone isn't confounded in any obvious way, not even partially. Thus, it appears to be causal as the internet people say. So does it explain the decline of testosterone? Probably in part. Let's recall what the obesity trend looks like:

There are longer running datasets, but they tell the same thing. The study that looked at the decline of testosterone actually tried controlling for BMI, and it did remove the trend:
Objective: The objective of the study was to examine whether an age-independent time trend in male serum testosterone levels exists.
Design and Setting: Testosterone and SHBG were analyzed in 5350 male serum samples from four large Danish population surveys conducted in 1982–1983, 1986–1987, 1991–1992, and 1999–2001. Free testosterone levels were calculated. The effects of age, year of birth, and time period on hormone levels were estimated in a general linear statistical model.
Main Outcome Measures: Testosterone, SHBG, and calculated free testosterone levels in Danish men in relation to age, study period, and year of birth were measured.
Results: Serum testosterone levels decreased and SHBG levels increased with increasing age. In addition to this expected age effect, significant secular trends in testosterone and SHBG serum levels were observed in age-matched men with lower levels in the more recently born/studied men. No significant age-independent effect was observed for free testosterone. Adjustment for a concurrent secular increase in body mass index reduced the observed cohort/period-related changes in testosterone, which no longer were significant. The observed cohort/period-related changes in SHBG levels remained significant after adjustment for body mass index.
Conclusions: The observed age-independent changes in SHBG and testosterone may be explained by an initial change in SHBG levels, which subsequently lead to adjustment of testosterone at a lower level to sustain free testosterone levels.
But only for testosterone, not for SHBG (Sex hormone-binding globulin), maybe that's important too, I don't know. So maybe the story is that obesity rates decrease testosterone, and this decrease causes the other manliness problems in men. That would be a simple, convenient theory. But I am tempted not to accept it entirely because we see a lot of these people these days:

As BMI is clearly not causal for these femboys, it seems we still need at least one secondary factor. Maybe something like this:
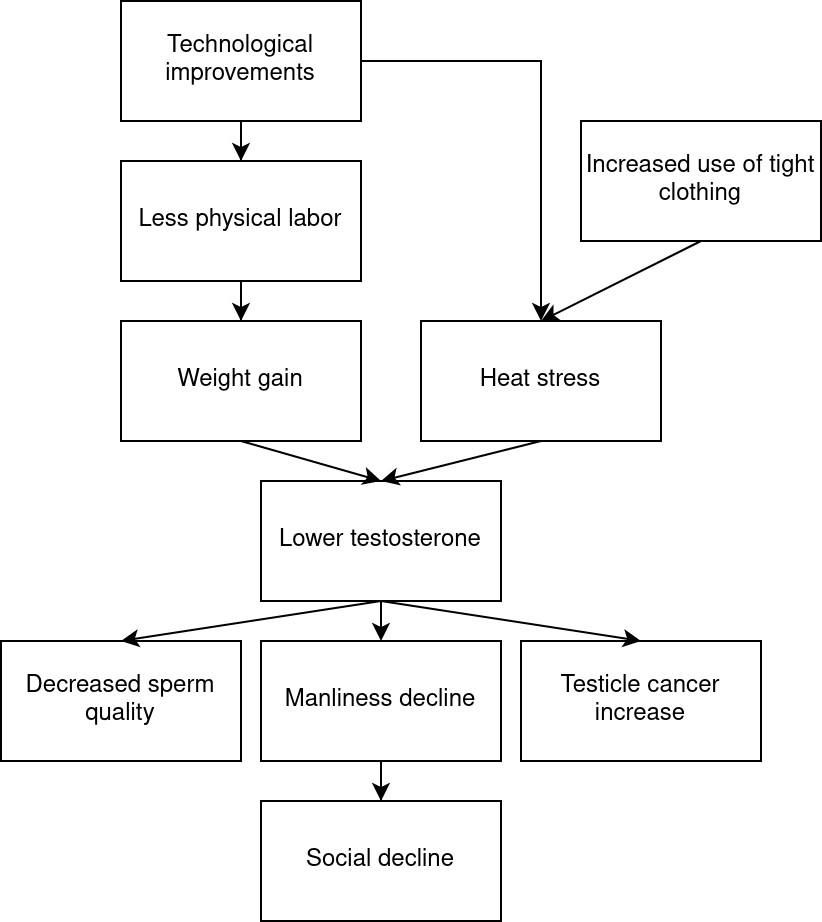
This model fits well with typical Uncle Ted takes, where technological progress is a kind of root cause of our problems.
Body fat doesn't absorb testosterone. It contains an enzyme (aromatase) that converts an androgen (androstenedione) into an estrogen (estrone). There have been many studies on the relationship between obesity in men and femininization, as well as between obesity in women and its moderating effects on menopause.
S. KIRCHENGAST, Interaction between sex hormone levels and body dimensions in postmenopausal women, Human Biology 66:481-494, 1994.
M.A. KIRSCHNER., G. Schneider, N.H. Ertel and E. Worton, Obesity, androgens, estrogens, and cancer risk, Cancer Research (suppl.) 42:3281-3285, 1982.
H.K. KLEY, T. Deselaers, H. Peerenboom and H.L. Krüskemper, Enhanced conversion of androstenedione to estrogens in obese males, Journal of Clinical Endocrinology and Metabolism 51:1128-1132, 1980.
H.K. KLEY, P. Edelmann and H.L. Krüskemper, Relationship of plasma sex hormones to different parameters of obesity in male subjects, Metabolism 29:1041-1045, 1980.
A. VERMEULEN and L. Verdonck, Factors affecting sex hormone levels in postmenopausal women, Journal of Steroid Biochemistry 11:899-904, 1979.
_____ and _____Sex hormone concentrations in post-menopausal women, Clinical Endocrinology 9: 59-66, 1978.
B. ZUMOFF, Relationship of obesity to blood estrogens, Cancer Research 42:3289-3294, 1982.
Adiposity has adaptive roots: it is a store of energy reserves, and it would aid reproduction in times of famine. Not only that, but the increasing BMI is a trend alongside many other adaptive traits trending globally across the 20th century, including such trends as increasing height, increasing longevity, increasing age at menopause, decreasing age at menarche, decreasing juvenile mortality, decreasing fertility, increasing intelligence, and increasing skull and brain sizes. This set of temporal trends also matches the cross-sectional direction from less-advantaged to more-advantaged countries. So, I think we should make sense of BMI more as an adaptive trait, less as a disease (though it is certainly a disease at the increasingly-common extremes), less as an unfortunate side effect.
BMI is a bit unusual among those adaptive traits because the temporal and country-level direction of covariance does not match the individual-level of covariance (age at menarche is another discrepancy). Among individuals in more-developed countries, the less-advantaged individuals have the greater BMI. In the least-developed countries, the covariance is in the expected direction, with the more-advantaged individuals having a greater BMI. This tells me what we already knew: apidosity is a calorie-overflow trait, in which calories are first allocated to the more important traits, and adiposity gets the leftovers.
I built a structural equation model and path diagram of such country-level traits. The model has excellent fit indices, and I found that BMI is caused by both juvenile survival and GDP per capita. So, those are the two most likely ultimate causes of both the country-level differences and the temporal differences.