
US BMI/obesity declined, but was it due to GLP-1?
Maybe some of it was COVID

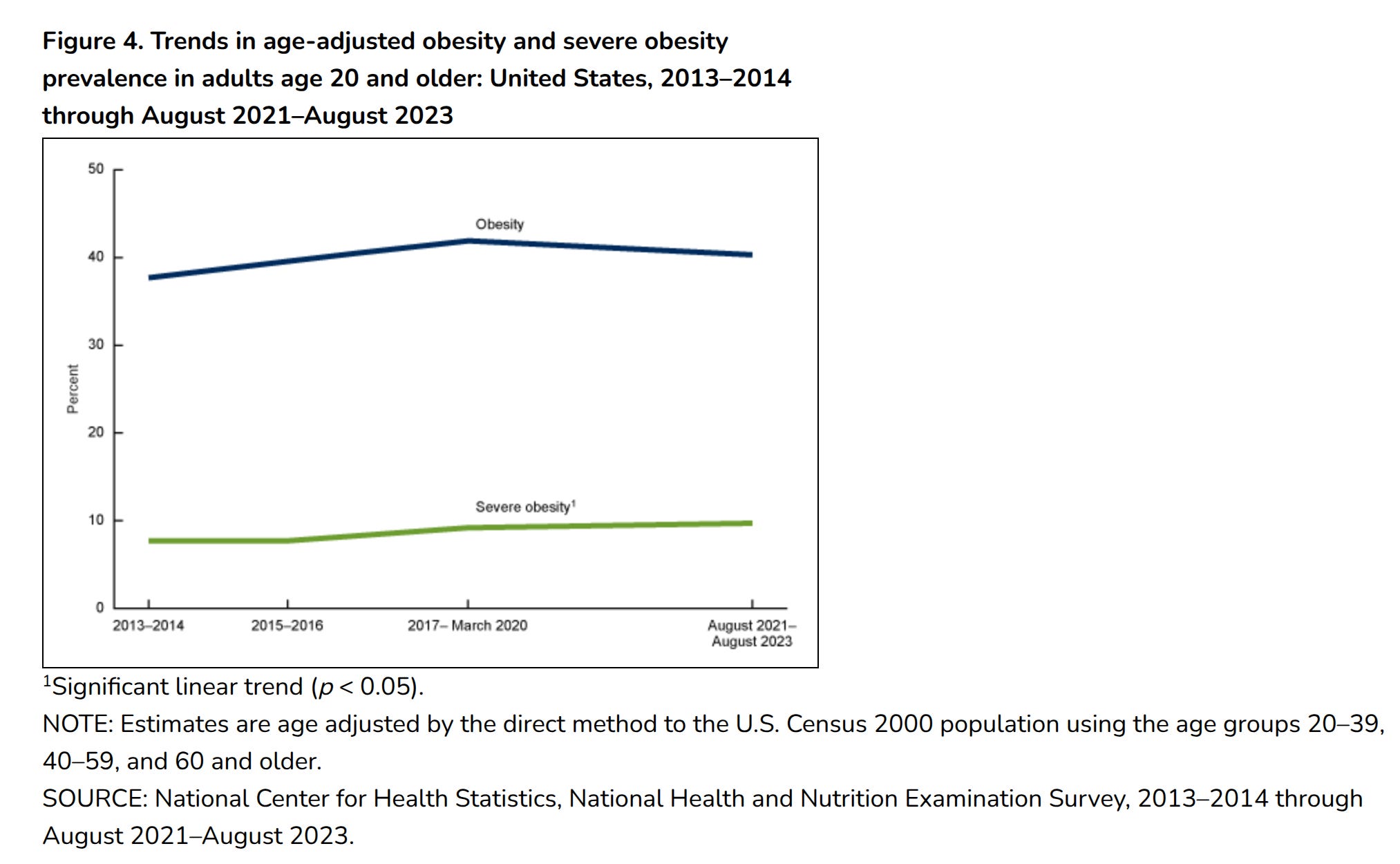
In tech circles, there has recently been many people cheering for the apparent success of Ozempic-like drugs (GLP-1 agonists) in finally reducing the American obesity rate. More and more variants of these drugs are coming out, each of them showing some apparent benefit over the previously. The CDC provides this plot based on the NHANES 2022:
And looking around, you will find that media headlines are based on another even larger study by Rader et al 2024:
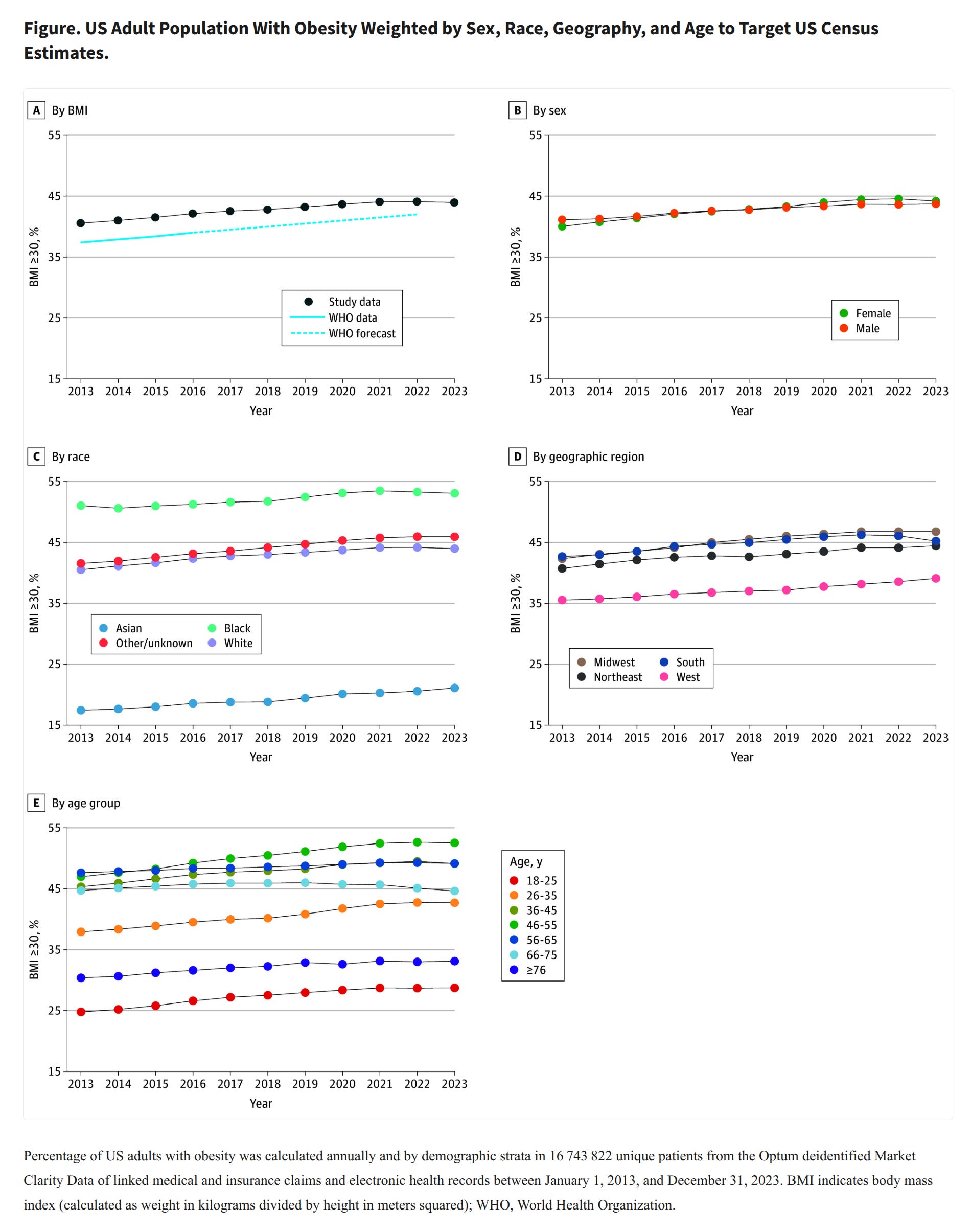
Rader et al provide more details of the trend by various subgroups. This is rather informative because it allows us to examine whether it is plausibly the weight loss drugs. As a matter of fact, looking at the age trends, there is only one group with a notable decline, the 66-75 year olds. Looking at the regions, there is only one with a notable decline, the US south. What factor operates particularly strongly in that particular combination? It's not drugs, but COVID:
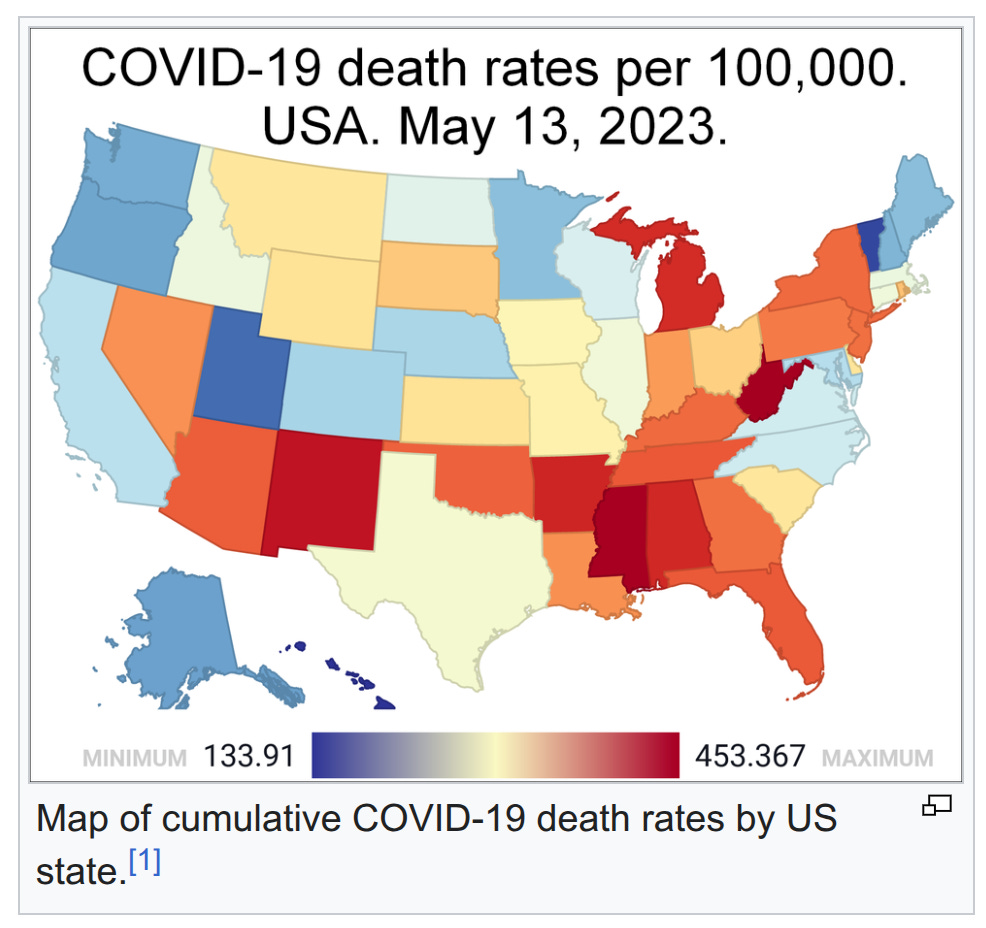
The same states have this kind of obesity level:
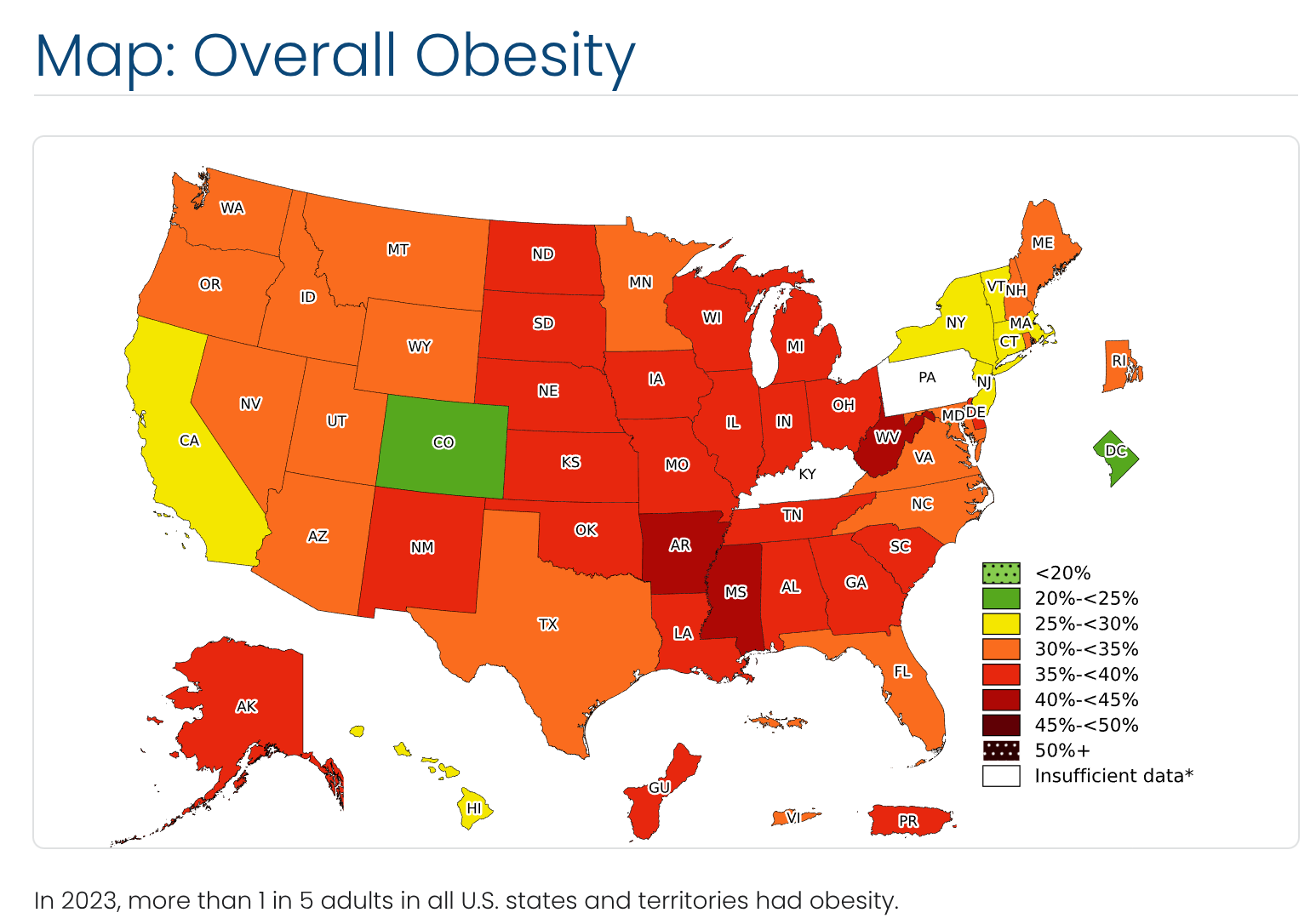
Note that Colorado sticks out because of the altitude effect. COVID of course killed more old people, and more obese people, and there are more of those in the south states. Such differential mortality means that the survivors will be lower in obesity, thus giving a decline.
Of course, these aggregate data considerations aren't conclusive, but the dataset isn't public, and I think the NHANES (which is public) is too small to model this, so there is little I can do here except to note that the authors agree with my speculations:
A decrease in obesity prevalence was observed in the South, among individuals aged 66 to 75 years, and among females (Figure, B-E). The 2023 decline in obesity prevalence was also seen in a sensitivity analysis using unweighted data (46.2%, 46.0%, and 45.6% in 2021, 2022, and 2023, respectively). For a subset of 10 625 745 individuals with available 2023 insurance claims, GLP-1RA dispensing differed by region (South, 6.0%; Midwest, 5.1%; Northeast, 4.4%; West, 3.4%).
These findings suggest that BMI and obesity prevalence in the US decreased in 2023 for the first time in more than a decade. The most notable decrease was in the South, which had the highest observed per capita GLP-1RA dispensing rate. However, dispensing does not necessarily mean uptake, and the South also experienced disproportionately high COVID-19 mortality among individuals with obesity.2
I think this slight difference in GLP-1 prescriptions is too small in absolute numbers to account for the difference seen.
There is another study by Lee et al 2024, showing some of the demographics of GLP-1 users. They results indicate that it is more commonly used in the south (the same as reported by Rader et al). More importantly, women use it more. Looking carefully at the obesity rate by sex, we see that women have a slight decline at the end of the time series, in line with this GLP-1 drug causation model, rather than COVID because men died more of COVID than women did (despite women being older). This is thus in support of the GLP-1 drug model instead of the COVID deaths. To note, the oldest age group of 75+ year olds did not see an obesity decline, which is not in line with selective mortality from COVID. There are no error bars so it is not entirely clear if we should make much of every tiny difference, even if their sample size is 17M people.
Perhaps further research can uncover which of these models is more correct for the COVID-era obesity decline, if it is indeed real at all. We have reason to doubt because the COVID years involved month long lockdowns that would have made representative medical measurements more difficult, and perhaps the slight decline is caused in part by sampling bias.
very nice observation and analysis. very plausible conclusion.