
Preferences can be sick: mental illness from an evolutionary perspective
A reply to Bryan Caplan and Scott Alexander

In the continuing debate about mental illness, we have roughly the following situation:
Bryan Caplan representing the Thomas Szasz camp
Scott Alexander representing the pragmatist "define mental illness in a way to benefit my friends" camp
And me, representing the evolutionary psychiatry camp
Here's some of the previous posts in the debate:
August 2006. The Economics of Szasz: Preferences, Constraints and Mental Illness (PDF)
30th May 2010. Diseased thinking: dissolving questions about disease
October 7, 2015. Contra Caplan on Mental Illness
Jan 6 2020. Scott Alexander on Mental Illness: A Belated Reply
Jan 15 2020. Contra Contra Contra Caplan On Psych
Jan 25, 2023. You Don't Want A Purely Biological, Apolitical Taxonomy Of Mental Disorders
Jan 26, 2023. Homosexuality is a mental illness
Jun 15, 2023. The Szaszian Fork: Another Reply to Scott Alexander on Mental Illness
Jun 29, 2023. Sure, Whatever, Let's Try Another Contra Caplan On Mental Illness
I may have missed some posts, but basically these two have been debating the topic for at least 8 years. I am a latecomer. Actually, I wasn't trying to enter their long-running debate, I merely wanted to bite the bullet that Scott Alexander presented in his post instead of taking his (to me) very strange political view of mental illness.
First, you might think I am straw-manning my opponents. Caplan is very straightforward about his views, e.g.:
If you’re paying attention, you know that I totally disagree with Emil. And you know why. To repeat: Preferences can’t be diseases! Not alcoholism, not idleness, not the urge to commit murder, and not your sexual preferences.
And here's Scott:
When the DSM is political, it’s not (just) because the authors are ideologues and want to go around stigmatizing people they don’t like. It’s because “is X a mental disorder or not?” is scientifically meaningless but politically very important.
...
The people asking for apolitical taxonomies want an incoherent thing. They want something which doesn’t think about politics at all, and which simultaneously is more politically correct than any other taxonomy.
Or if “political correctness” sounds too dismissive, we can rephrase it as: “they want something that doesn’t think about ethics and practicality at all, but which is simultaneously more ethically correct and pragmatically correct than other taxonomies”. That is, we want our definition of “mental disorder” to be ethical (eg not stigmatize people who don’t deserve stigma). And we want it to be practical (eg identify a group of people who need and deserve care). But things that are biologically similar can be ethically and practically different
Call me naive or an idealist, but I would like that scientific concepts not depend on arbitrary political decisions, and especially not those of a sick country like America. Scott and Caplan are actually somewhat in agreement that taxonomies are meaningless, but Scott just wants to keep them in order to get funding for his friends, while Caplan presumably wants to abolish public support for psychiatry (per his libertarian stance).
Since I received some criticism for not going fully into the debate about how to define or think about mental illness in my last post, I guess I can do it here. I think good science is reductive, like this:
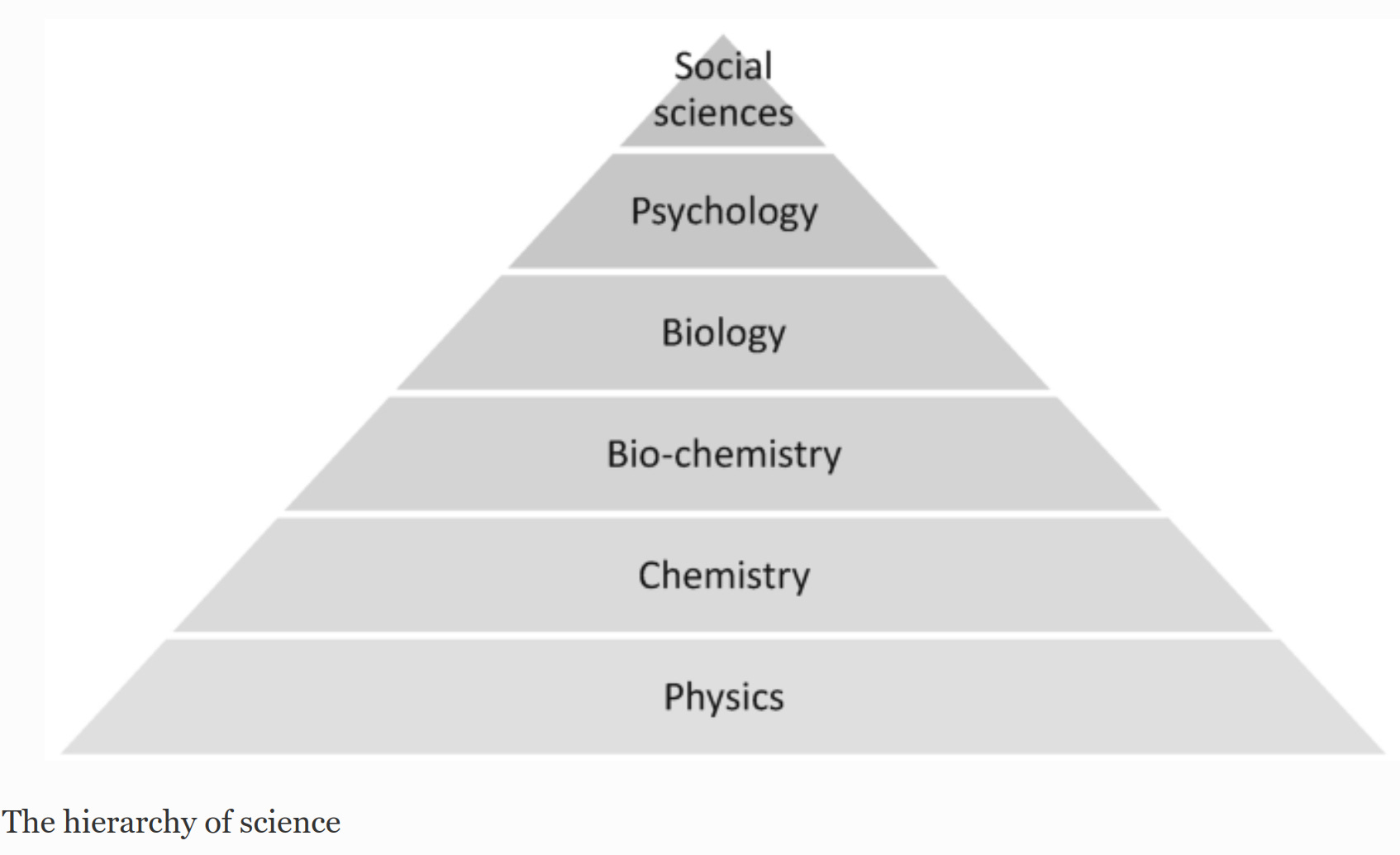
So chemistry is large-scale physics, biology is large-scale chemistry, etc. in order of increasing complexity. As you move on the hierarchy, new phenomena emerge that would be silly to describe using only the concepts of the underlying level, even if it is in principle possible (you could describe evolution by talking about particles, but that would be very complicated). Most people agree with this until we get to human psychology. From the reductionist perspective, humans are biological creatures like any other species, so their behavior must be explained by reference to more general mechanisms common to primates, mammals, and life in general. This meta-theory of psychology is called evolutionary psychology, or sociobiology originally until the socialists gave this a bad name). I take it for granted that readers of this blog will be familiar with evolutionary psychology in general, which is a very broad field. One part that is less written about is evolutionary psychiatry. In fact, the reason I started thinking about this was Scott's own 2018 post reviewing a book with the title, Evolutionary Psychopathology by Marco Del Giudice. It's a fascinating attempt at linking together all the various aspects of life history theory with psychiatry. Bold and probably wrong in many ways, it is nevertheless the only such broad attempt I'm familiar with. So if Scott is unhappy with me biting his bullet, he should know that he himself caused this!
From an evolutionary perspective, animals adapt to their environments. They do this not because of God guiding evolution, or because animals just try harder over time. They do it because the animals that are less fit to the environment die off, leaving descendants with genetic variants who are marginally better functioning in that environment. In that sense, evolution by natural selection is a blind, stupid method that leads to an increasingly better fit between the genetic variants and the organism they code for and the environment over time.
From this perspective, we can talk about maladaptive behavior, which is the result of maladaptive psychological traits. Whether these are preferences or not is moot, it doesn't matter what we call them. I guess preferences are given a special role by Caplan because much economics theory is built around rational agents models, which has preferences in a key role. In non-psychological medicine, we talk about diseases, mainly when we mean infectious diseases. These are relatively straightforward to think about because they involve a foreign (non-human) agent causing problems in the body, whether this is the influenza virus, cholera bacteria, or intestinal parasites doesn't matter so much. There are some infections that target the brain or nervous system and affect behavior, but these are pretty rare. Mostly people talk about Toxoplasma gondii, but those effects are pretty dubious in humans, even if they are well-established in cats. The more broad category of diseases is disorders, which as the word suggests, is some kind of deviation from order, or how the body is supposed to work. Supposed here meaning that the body works in the way evolution designed it to solve the problems it faces. We consider heart disease a problem because the function of the heart is to pump oxygenated blood around and when it fails to do so, bad things will follow, usually pain and death. Generally, heart disease isn't caused by a foreign agent (but it can be, such as coronavirus and the vaccines), so I guess heart disorder would be a more appropriate term.
In this framework, mental disorders are not too much different from physical disorders. They are some kind of deviation from the optimal functioning. These can be in many domains. For instance, humans have food preferences that are fairly consistent. We like fatty food, sweet food, and we don't in general like very bitter, sour, or otherwise foul tasting foods. This is intended because such foods can be poisonous or just plainly non-nutritious. So to avoid them, humans involved certain built-in preferences to help guide behavior. These are not exactly strict, as many people like some level of sourness (e.g. lemon spice), and some like bitterness (e.g. beer, or bitter lemon). The preference for sweetness is probably related to the ripeness of fruits, as that's when they are in the most nutritious stage of their life cycle. Bitter means unripe (not ready to eat), and rotten is overripe (can be poisonous). If someone's preferences are severely deviating from this general pattern, we call it a disorder. If someone prefers eating human feces to eating a banana, there is surely something very wrong with them. One common problem in this direction is pica:
Pica is the eating or craving of things that are not food.[2] It can be a disorder in itself or medical phenomena. The ingested or craved substance may be biological, natural or manmade. The term was drawn directly from the medieval Latin word for magpie, a bird subject to much folklore regarding its opportunistic feeding behaviors.[3]
According to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), pica as a standalone eating disorder must persist for more than one month at an age when eating such objects is considered developmentally inappropriate, not part of culturally sanctioned practice, and sufficiently severe to warrant clinical attention. Pica may lead to intoxication in children, which can result in an impairment of both physical and mental development.[4] In addition, it can cause surgical emergencies to address intestinal obstructions, as well as more subtle symptoms such as nutritional deficiencies and parasitosis.[4] Pica has been linked to other mental disorders. Stressors such as psychological trauma, maternal deprivation, family issues, parental neglect, pregnancy, and a disorganized family structure are risk factors for pica.[4][5]
Pica is most commonly seen in pregnant women,[6] small children, and people who may have developmental disabilities such as autism.[7] Children eating painted plaster containing lead may develop brain damage from lead poisoning. A similar risk exists from eating soil near roads that existed before the phase-out of tetraethyllead or that were sprayed with oil (to settle dust) contaminated by toxic PCBs or dioxin. In addition to poisoning, a much greater risk exists of gastrointestinal obstruction or tearing in the stomach. Another risk of eating soil is the ingestion of animal feces and accompanying parasites. Cases of severe bacterial infections occurrence (leptospirosis) in patients diagnosed with pica have also been reported.[8] Pica can also be found in animals such as dogs[9] and cats.[10]
It can get extreme:

Stomach contents of a psychiatric patient with pica: 1,446 items, including "457 nails, 42 screws, safety pins, spoon tops, and salt and pepper shaker tops".
Caplan would have to claim that pica isn't a disorder, but just one weird food preference among others. Pica can kill you, of course, but evidently the patient above managed to eat ~1500 items without dying.
In a similar vein, eating too little food will kill you. That's why we consider these also to be eating disorders. There are various ways to classify these based on the clusters of behaviors, but most people talk about anorexia and bulimia. Sometimes the media will feature some person who has extreme pickiness, which is also suboptimal but in a modern environment it is generally possibly to function by eating only chocolate.

Caplan would say this girl just has a weird preference, but in reality she's a big strain on her parents due to the unusual diet, which in this case, has its cause in autistic fear of trying new things.
You can see where this is going perhaps. With regards to sexuality, humans are a sexually reproductive species, meaning that we have two sexes and they have to have sex to reproduce. Specifically, they must have vaginal intercourse ending with ejaculation. As such, if one deviates from this norm, it will have some kind of cost. One can deviate within heterosexual norms, for instance, by having strong preferences for non-vaginal sex (oral, anal, feet, hands, masturbation etc.), by being interested in the wrong sex (homosexuality, or bisexuality), or the wrong age range. Some unusual people deviate so far as to be having sex with the wrong species (horses, dogs, goats, sheep, cats etc.). It is clear from discussion of these that being disordered is a matter of degree. Preferences for oral sex presumably evolved in humans because this has other benefits for pair-bonding, while not having a too high fertility cost. Every time one has non-vaginal sex, one could have been having vaginal sex instead, which can lead to pregnancy. As non-vaginal sex never leads to pregnancy there is an opportunity cost of this. However, if this cost isn't great, the fitness cost of non-vaginal sex is not large, and it only becomes a problem if it's extreme. One might even speculate that women evolved to provide non-vaginal sex for situations where they do not want pregnancy to occur but still want to acquire some other benefit from a man, or to build towards future partnership. One can find many papers speculating about these things, and many of them of course apply to both sexes (cheating detection, mate-retention). Various preferences for sex positions (missionary, doggy-style, standing etc.) do not seem to relate to pregnancy chances, so unless they have some other major cost, can not be considered disordered in some sense.
We can generalize some of the above by classifying preferences into those relating to sexual targeting, or who one has a preference for having sex with. For reproduction to occur, these must be opposite sex at the appropriate age (and timing of the female cycle, a preference for sex at menstruation would be maladaptive, and indeed, most people avoid this). The further one deviates from this, the more disordered the preference is. As such, strict homosexuality is more disordered than bisexuality. There's nothing wrong with using sex for non-reproductive purposes, as both bonobos and humans do, and probably other species (e.g. dolphins). But since time is limited, each such act has some opportunity cost, and thus if extreme would be disordered. In general, then, all sexual disorders are a matter of degree with a large zone of variation that cannot be considered disordered. We can visualize it like this:

The main dimensions that one can deviate along are:
Sex of partner: healthy = opposite sex, maximal disordered = exclusively same sex
Age of partner: for men, fertile females (roughly 15-45), for women, 15+. Strong preferences for outside of these ranges would be disordered
Species: healthy = humans, disordered = any other species
Sexual activity: healthy = vaginal, strong preference for anything else = disordered
Family members: healthy = non-close family members, close family members = disordered
For any given individual, then, one can compute a sexual deviance, or disorder, score by summing the difference from the maximally adaptive preferences. On this model, there are no strict categories, but we can label various parts of this preference space for organizational purposes. We call men gay if they only have sex with other men. We call people pedophiles if they are mainly interested in sex with prepubescents. We call it bestiality if people are interested in having sex with animals.
The purpose of this scientific way of thinking about human sexuality is not to try to get governments to pay for treatment of people (if any such exists or works), but just as a matter of thinking about how the world works. I submit that this is the chief function of science. Probably if we had effective treatment for altering someone's preferences towards the healthy area, many people would be eager to get it. Presumably before society made homosexuality a cool thing to be, many people sought treatment for same-sex preferences.
On a practical note, since it is an empirically well-established finding that mental disorders are statistically associated with each other, we can use this to help figure out what is disordered and what is not. Simply, whatever correlates strongly with other disorders is a prime candidate for itself being a disorder of some sort. On this model, then, finding that the genetic variants that make someone a homosexual, transsexual, pedophile also make them depressed, anxious etc. is evidence for these being a disorder. But this is only a pragmatic matter, as the definition comes from its evolutionary implications, not this empirical fact of general covariance.
This approach to mental disorders has the usual set of objections. It used to be popular to be a monk or a nun. Since they are forbidden from having sex and children, this is surely maladaptive behavior. Should this be considered disordered? I bite the bullet and say yes. But it wasn't too common either, probably less than 1% of the population even at its medieval height. It can be considered a kind of religious overreach. Religiousness is generally pro-natalist, but some variants can be anti-natalist, and thus maladaptive. Similarly, the modern day equivalent of being an anti-natalist is maladaptive and a disorder. Indeed, anti-natalism probably correlates with various regular mental illnesses. I wasn't able to find a study (but one can look it up in the OKCupid dataset), however, we can take a first stab at this question by looking at our trusted subreddit overlap calculator:

There's 4 mental illness subreddits among the top, with very high rates of over-representation. There's also a bunch of sad or antisocial leftist reddits (e.g. antiwork), which we already know are associated with mental illness.
Conclusions
Based on a reductionist, evolutionary perspective, preferences that deviate strong from appropriate age, human heteronormativity are sick or maladaptive. This is a matter of degree, not either/or.
One can bite the bullet and agree that long-term sexual abstinence or anti-natalism views and behaviors are also sick. They show the usual positive manifold with other more recognized problems (e.g. depression).
There is no need to inject politics into the scientific study of mental illnesses, in the same way we don't inject politics into the study of many other natural phenomena.
These conclusions aren't so bad from a classical liberal perspective. Just because we recognize that such behaviors are disordered, doesn't mean they should be criminal or legal. That would depend on the usual harm considerations. Likewise, treatment options should be allowed and probably subsidized by the state (if it's in the business of doing healthcare that is). I see no reason to force treatment in the same way we don't force someone to get their broken bones fixed, or cancer cured.
This framework isn't that radical. It's simply implying that psychiatrists were right about homosexuality and transgenderism until recently, and they were pushed by activism from these minorities to declassify them for non-scientific reasons.
Of course, I don't claim this is a water-tight philosophical case for this framework. This is just a sketch so that one can get the general idea of the evolutionary psychiatric perspective, and the details can be fleshed out with regards to sexual disorders if someone is interested in doing that.
Does anyone know a good psychologist who could help me get through my issues? I suffer from long-term sexual abstinence. I am looking for the following qualifications: female, 18-25, preferably blond
Randolph Nesse also has a book on evolutionary psychiatry btw
https://www.amazon.com/Good-Reasons-Bad-Feelings-Evolutionary/dp/1101985666